Hypertension, drug classes, causes, symptoms, treatment, foods, brand generic drugs
Table of Contents
Hypertension
Hypertension, commonly known as high blood pressure, is a chronic medical condition where the force of blood against the walls of the arteries is consistently too high. Over time, this can damage blood vessels and lead to serious health complications.
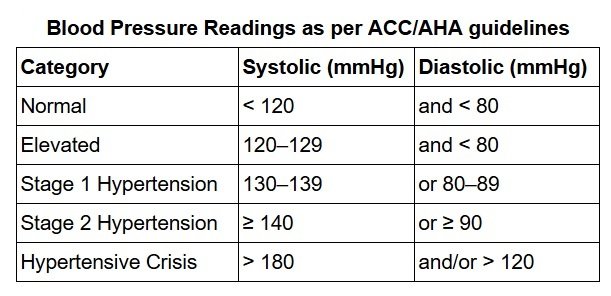
Blood Pressure Readings
Blood Pressure is measured as systolic pressure (top number) over diastolic pressure (bottom number) in mmHg.
- Normal: <120/80 mmHg
- Elevated: 120–129/<80 mmHg
- Hypertension Stage 1: 130–139/80–89 mmHg
- Hypertension Stage 2: ≥140/90 mmHg
- Hypertensive Crisis: >180
Types of Hypertension
- Primary (Essential) Hypertension (90–95% of cases): No identifiable cause, develops gradually due to genetics, lifestyle, or aging.
- Secondary Hypertension (5–10% of cases): Caused by an underlying condition (e.g., kidney disease, hormonal disorders, medications).

Causes of Hypertension (High Blood Pressure)
Hypertension (HTN) is classified into primary (essential, 90-95% of cases) and secondary (5-10%), where an underlying condition is the cause. Below are the major causes:1. Primary (Essential) Hypertension
No single identifiable cause; results from a combination of genetic, lifestyle, and environmental factors:- Genetics (family history)
- Obesity (↑ adipokines, insulin resistance)
- High salt intake (Na⁺ retention → ↑ blood volume)
- Alcohol & tobacco use (vasoconstriction)
- Sedentary lifestyle (↓ vascular health)
- Chronic stress (↑ sympathetic activity)
- Aging (arterial stiffness)
2. Secondary Hypertension (Underlying Causes)
A. Kidney-Related
- Chronic kidney disease (CKD) (↓ Na⁺ excretion)
- Renal artery stenosis (↑ renin → angiotensin II → vasoconstriction)
- Polycystic kidney disease
B. Endocrine Disorders
- Primary hyperaldosteronism (Conn’s syndrome – excess aldosterone)
- Cushing’s syndrome (excess cortisol → Na⁺ retention)
- Pheochromocytoma (catecholamine-secreting tumor → episodic HTN)
- Hyperparathyroidism (↑ Ca²⁺ → vascular stiffness)
- Hyper/hypothyroidism
C. Cardiovascular & Vascular
- Aortic coarctation (narrowing of the aorta)
- Obstructive sleep apnea (hypoxia → sympathetic overdrive)
D. Medications & Substances
- NSAIDs (↓ prostaglandin-mediated vasodilation)
- Oral contraceptives (estrogen-induced fluid retention)
- Decongestants (pseudoephedrine → vasoconstriction)
- Steroids (corticosteroids, anabolic steroids)
- Cocaine/amphetamines (sympathetic overstimulation)
E. Other Causes
- Pregnancy-induced HTN (preeclampsia)
- Liquorice abuse (glycyrrhizin → pseudoaldosteronism)
Risk Factors for Hypertension
| Non-Modifiable | Modifiable |
| Age (↑ risk after 40) | Obesity (BMI ≥30) |
| Family history | High-sodium diet |
| Male gender (pre-menopause women have lower risk) | Alcohol excess |
| Black/African descent | Physical inactivity |
| Chronic stress | |
Low potassium intake |
Types of Antihypertensive Medications
Antihypertensive drugs are classified based on their mechanism of action.The major classes include:
- ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors) (Blocks angiotensin II production, dilate blood vessels)
- ARBs (Angiotensin II Receptor Blockers) (Block angiotensin II receptors, similar to ACEIs but no cough)
- Calcium Channel Blockers (CCBs) (Relax blood vessels by blocking calcium entry into muscle cells)
- Alpha-Blockers (Block alpha-1 receptors, dilate blood vessels)
- Beta-Blockers (Reduce heart rate and cardiac output)
- Centrally Acting Agents (Reduce sympathetic nervous system activity)
- Vasodilators (Directly relax arterial smooth muscle)
- Diuretics (Reduce blood volume by increasing urine output)
First-Line Treatment Choices (JNC 8 & ACC/AHA Guidelines)
- General population: ACEI/ARB + CCB or Thiazide Diuretic.
- Black patients: CCB or Thiazide Diuretic (ACEIs/ARBs less effective alone).
- Heart disease patients: Beta-blockers + ACEI/ARB.
- Chronic kidney disease (CKD): ACEI/ARB (renal protective).
ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors)
| Brand Name | Generic Name | Mechanism of Action | Common Side Effects |
| Zestril, Prinivil | Lisinopril | Inhibits angiotensin-converting enzyme (ACE), reducing angiotensin II production and aldosterone secretion → vasodilation and decreased BP | Dry cough, hyperkalemia, angioedema, hypotension, dizziness |
| Vasotec | Enalapril | ||
| Altace | Ramipril | ||
| Accupril | Quinapril | ||
| Lotensin | Benazepril | ||
| Monopril | Fosinopril | ||
| Mavik | Trandolapril | ||
| Capoten | Captopril | Short-acting ACE inhibitor, same MOA | Taste disturbances, rash, proteinuria, same as others |
Combination ACE Inhibitor Drugs | |||
| Zestoretic | Lisinopril / Hydrochlorothiazide (HCTZ) | ACE inhibition + thiazide diuretic →↓ RAAS activity + ↑ sodium/water excretion | Dry cough, hyperkalemia, hypotension, electrolyte imbalance |
| Vaseretic | Enalapril / HCTZ | ||
| Lotensin HCT | Benazepril / HCTZ | ||
| Accuretic | Quinapril / HCTZ | ||
| Monopril HCT | Fosinopril / HCTZ | ||
| Uniretic (some regions) | Moexipril / HCTZ | ||
| Tarka | Trandolapril / Verapamil | ACE inhibition + calcium channel blockade → vasodilation + ↓ HR | Bradycardia, constipation, cough, hyperkalemia |
How ACE Inhibitors Work:
ACE (angiotensin-converting enzyme) inhibitors are a class of drugs primarily used to treat hypertension (high blood pressure) and heart failure.Their mechanism of action involves:
Blocking Angiotensin-Converting Enzyme (ACE):
- Normally, ACE converts angiotensin I → angiotensin II (a potent vasoconstrictor).
- ACE inhibitors prevent this conversion, reducing angiotensin II levels.
Effects of Reduced Angiotensin II:
- Vasodilation: Less angiotensin II → relaxed blood vessels → lower blood pressure.
- Decreased Aldosterone Secretion: Reduces sodium/water retention → less fluid volume & lower BP.
- Reduced Cardiac Remodeling: Protects the heart in heart failure by preventing harmful tissue changes.
Increased Bradykinin Levels:
- ACE also breaks down bradykinin (a vasodilator).
- Inhibiting ACE increases bradykinin, enhancing vasodilation (but may cause dry cough as a side effect).
Side Effects of ACE Inhibitors:
- Dry cough (bradykinin-related)
- Hyperkalemia (high potassium)
- Angioedema (rare but serious)
- Hypotension (first-dose effect)
ARBs (Angiotensin II Receptor Blockers)
| Brand Name | Generic Name | Mechanism of Action | Common Side Effects |
| Cozaar | Losartan | Blocks angiotensin II from binding to AT1 receptors → vasodilation, ↓ aldosterone | Hyperkalemia, dizziness, fatigue, hypotension |
| Diovan | Valsartan | Hyperkalemia, headache, dizziness | |
| Benicar | Olmesartan | Hyperkalemia, dizziness, rare: sprue-like enteropathy | |
| Avapro | Irbesartan | Hyperkalemia, dizziness, fatigue | |
| Micardis | Telmisartan | Hyperkalemia, back pain, dizziness | |
| Atacand | Candesartan | Hyperkalemia, hypotension, dizziness | |
| Teveten | Eprosartan | Hyperkalemia, headache, cough, dizziness | |
| Edarbi | Azilsartan | Hyperkalemia, diarrhea, increased serum creatinine | |
ARB Combination Drugs (ARB + Thiazide) | |||
| Hyzaar | Losartan + HCTZ | Vasodilation + ↑ Na/H2O excretion | Dizziness, hypokalemia, hyperuricemia, hyperkalemia |
| Diovan HCT | Valsartan + HCTZ | Dizziness, fatigue, electrolyte imbalance | |
| Benicar HCT | Olmesartan + HCTZ | Dizziness, hyperuricemia, dry mouth | |
| Avalide | Irbesartan + HCTZ | Headache, fatigue, hypokalemia | |
| Micardis HCT | Telmisartan + HCTZ | Dizziness, upper respiratory infection | |
| Atacand HCT | Candesartan + HCTZ | Hypotension, back pain, dizziness | |
| Teveten HCT | Eprosartan + HCTZ | Fatigue, headache, cough | |
| Edarbyclor | Azilsartan + Chlorthalidone | Increased uric acid, dizziness, diarrhea | |
How ARBs (Angiotensin II Receptor Blockers) Work
ARBs (e.g., Losartan, Valsartan, Irbesartan) are another key class of antihypertensive drugs, often used as an alternative to ACE inhibitors.Mechanism of Action:
Block AT1 Receptors:
- ARBs selectively block angiotensin II (Ang II) receptors (AT1 subtype).
- Unlike ACE inhibitors, they do not affect bradykinin metabolism (hence, no dry cough).
Effects of AT1 Blockade:
- Vasodilation: Prevents Ang II-induced vasoconstriction → lowers blood pressure.
- Reduced Aldosterone Release: Decreases sodium/water retention → reduces blood volume.
- Cardiac & Renal Protection: Slows heart failure progression and diabetic nephropathy (similar to ACE inhibitors).
Key Notes for Pharmacy Students
- ARB + HCTZ combinations enhance BP control through dual mechanisms.
- Avoid in pregnancy (Category D).
- Monitor: BP, potassium, renal function, signs of hypotension.
- No cough, unlike ACE inhibitors (no bradykinin effect).
- Watch for hyperkalemia, especially with potassium supplements or potassium-sparing diuretics.
Side Effects of ARBs:
- Hyperkalemia (high potassium)
- Dizziness/Hypotension (especially in volume-depleted patients)
- Angioedema (rare, but less than ACE inhibitors)
- Teratogenic (avoid in pregnancy, like ACE inhibitors)
ACE Inhibitors vs ARBs Comparison
| Feature | ACE Inhibitors | ARBs (Angiotensin II Receptor Blockers) |
| Mechanism of Action | Inhibit Angiotensin-Converting Enzyme (ACE), preventing conversion of Angiotensin I → II | Block Angiotensin II from binding to AT1 receptors |
| Bradykinin Effects | ↑ Bradykinin (leads to cough, angioedema) | No effect on bradykinin (less cough, lower risk of angioedema) |
| Cough | Common side effect (up to 20%) | Rare |
| Angioedema | More common | Less common |
| Preferred in | Diabetic nephropathy, post-MI, HF (with reduced EF) |
Patients who can’t tolerate ACE inhibitors (due to cough or angioedema)
|
| Side Effects | Cough, angioedema, hyperkalemia, hypotension, ↑ creatinine | Hyperkalemia, hypotension, dizziness |
| Contraindications | Pregnancy, bilateral renal artery stenosis, angioedema history | Same as ACE inhibitors |
| Combination with NSAIDs and Diuretics | ↑ Risk of AKI with both classes (Triple Whammy: ACEi + NSAID + Diuretic) | Same risk with ARBs |
| Monitoring | Potassium, renal function, BP | Same as ACE inhibitors |
Calcium Channel Blockers (CCBs) Antihypertensive Drugs
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
| Dihydropyridine | |||
| Norvasc | Amlodipine | Dihydropyridine CCB: Blocks L-type calcium channels in vascular smooth muscle → vasodilation | Peripheral edema, dizziness, flushing, palpitations |
| Procardia, Adalat CC | Nifedipine | Dihydropyridine CCB: Vasodilation via L-type calcium channel blockade | Headache, flushing, reflex tachycardia, edema |
| Plendil | Felodipine | Dihydropyridine CCB: Vasodilation | Swelling, headache, fatigue |
| Sular | Nisoldipine | Dihydropyridine CCB: Vasodilation | Edema, dizziness, flushing |
| Cardene | Nicardipine | Dihydropyridine CCB: Vasodilation | Hypotension, headache, tachycardia |
| Non-Dihydropyridine | |||
| Isoptin, Calan, Verelan | Verapamil | Non-Dihydropyridine CCB: Slows AV node conduction and myocardial contractility | Constipation, bradycardia, heart block, gingival hyperplasia |
| Cardizem, Tiazac | Diltiazem | Non-Dihydropyridine CCB: Negative chronotrope and inotrope | Bradycardia, dizziness, edema |
Combination Calcium Channel Blockers Antihypertensive Drugs | |||
| Exforge | Amlodipine + Valsartan | CCB + ARB | Edema, dizziness, fatigue |
| Twynsta | Amlodipine + Telmisartan | CCB + ARB | Edema, back pain, dizziness |
| Azor | Amlodipine + Olmesartan | CCB + ARB | Edema, hypotension, dizziness |
| Tribenzor | Amlodipine + Olmesartan + HCTZ | CCB + ARB + Thiazide | Dizziness, hyperuricemia, electrolyte imbalance |
| Exforge HCT | Amlodipine + Valsartan + HCTZ | CCB + ARB + Thiazide diuretic | Dizziness, fatigue, hyperkalemia, hypotension, dehydration |
| Lotrel | Amlodipine + Benazepril | CCB + ACE inhibitor | Cough, edema, hyperkalemia, dizziness |
| Prestalia | Amlodipine + Perindopril | CCB + ACE inhibitor | Cough, dizziness, peripheral edema |
| Tekamlo | Amlodipine + Aliskiren | CCB + Direct Renin Inhibitor | Diarrhea, hypotension, hyperkalemia (avoid in pregnancy) |
| Amturnide | Amlodipine + Aliskiren + HCTZ | CCB + Direct Renin Inhibitor + Thiazide | Fatigue, dizziness, electrolyte disturbances |
Types of CCBs
| Class | Examples | Primary Effects | Main Uses |
|---|---|---|---|
| Dihydropyridines (DHPs) | Amlodipine, Nifedipine | Strong vasodilation, minimal cardiac effect | Hypertension, Angina |
| Non-Dihydropyridines | Verapamil, Diltiazem | Cardiac depression + moderate vasodilation | Arrhythmias, Angina |
How Calcium Channel Blockers (CCBs) Work
Calcium channel blockers (CCBs) are a class of drugs used primarily for hypertension (high blood pressure), angina (chest pain), and arrhythmias (irregular heartbeats). They work by blocking voltage-gated calcium channels (L-type), reducing calcium influx into cells, which affects vascular smooth muscle and cardiac muscle differently.
Mechanism of Action
In Blood Vessels (Vasodilation):
- CCBs block calcium entry into vascular smooth muscle cells.
- ↓ Intracellular calcium → relaxes arteries → reduces peripheral resistance → lowers blood pressure.
- This helps treat hypertension and vasospastic angina.
In the Heart:
- Dihydropyridines (e.g., Amlodipine, Nifedipine):
- Mostly affect blood vessels (minimal cardiac effect).
- Non-Dihydropyridines (e.g., Verapamil, Diltiazem):
- Also block calcium channels in the heart, leading to:
- ↓ SA node firing (↓ heart rate – negative chronotropy).
- ↓ AV node conduction (↓ heart rate – negative dromotropy).
- ↓ Myocardial contractility (↓ force – negative inotropy).
- Also block calcium channels in the heart, leading to:
- Useful for supraventricular arrhythmias and chronic stable angina.
Side Effects of Calcium Channel Blockers
Dihydropyridines:
- Reflex tachycardia (due to vasodilation)
- Peripheral edema (ankle swelling)
- Headache, flushing
Non-Dihydropyridines:
- Bradycardia (slow heart rate)
- Constipation (Verapamil)
- AV block (caution in heart failure)
Alpha Blockers – Antihypertensive Drugs
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
Selective Alpha Blockers |
|||
| Cardura | Doxazosin | Selective α1-blocker: Relaxes vascular smooth muscle → vasodilation | Orthostatic hypotension, dizziness, headache, fatigue |
| Minipress | Prazosin | Selective α1-blocker: Lowers peripheral resistance | First-dose hypotension, dizziness, nasal congestion |
| Hytrin | Terazosin | Selective α1-blocker: Vasodilation and reduced blood pressure | Drowsiness, postural hypotension, syncope |
| Uroxatral | Alfuzosin | Selective α1-blocker: Primarily used for BPH but may have BP-lowering effects | Dizziness, orthostatic hypotension |
| Rapaflo | Silodosin | Selective α1A-blocker (more prostate-specific, minimal BP effect) | Retrograde ejaculation, dizziness |
| Flomax | Tamsulosin | Selective α1A-blocker (for BPH; not used for BP) | Dizziness, ejaculatory dysfunction |
Non-Selective Alpha Blockers |
|||
| Regitine | Phentolamine | Non-selective α1/α2-blocker: Vasodilation, used for hypertensive emergencies, pheochromocytoma | Reflex tachycardia, GI upset, hypotension |
| Phenoxybenzamine | Phenoxybenzamine | Irreversible non-selective α1/α2-blocker: Pre-op pheochromocytoma management | Postural hypotension, nasal stuffiness, tachycardia |
How Alpha Blockers Work
- Block α₁-receptors on vascular smooth muscle → vasodilation → ↓ peripheral resistance → ↓ blood pressure.
- In the prostate/bladder neck, they relax smooth muscle → improve urine flow (used for BPH).
A. Hypertension
- Not first-line (JNC8 & ACC/AHA guidelines prefer thiazides, ACEIs, ARBs, or CCBs).
- Used in resistant hypertension (added to other drugs).
- Preferred in patients with comorbid BPH (helps both conditions).
B. Benign Prostatic Hyperplasia (BPH)
- Improves urinary symptoms by relaxing prostate/bladder neck muscles.
C. Pheochromocytoma
- Phenoxybenzamine/phentolamine used preoperatively to prevent catecholamine-induced hypertension.
Side Effects of Alpha Blockers
- First-dose hypotension (dizziness, syncope – minimized by starting at bedtime).
- Reflex tachycardia (due to vasodilation; often requires a beta-blocker).
- Dizziness, fatigue, nasal congestion.
- Orthostatic hypotension (higher risk in elderly).
Beta Blockers – Antihypertensive Drugs
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
Selective Beta-1 Blockers (Cardioselective) |
|||
| Tenormin | Atenolol | Selective β1 blocker → ↓ heart rate, ↓ contractility, ↓ renin release (less preferred today) | Bradycardia, fatigue, dizziness, cold extremities |
| Lopressor | Metoprolol tartrate | Selective β1 blocker → short-acting | Bradycardia, fatigue, hypotension |
| Toprol XL | Metoprolol succinate | Selective β1 blocker → extended release | Drowsiness, depression, bradycardia |
| Bystolic | Nebivolol | Selective β1 blocker + nitric oxide–mediated vasodilation (vasodilatory effects (NO-mediated) | Headache, dizziness, bradycardia |
| Zebeta | Bisoprolol | Highly selective β1 blocker (preferred for heart failure) | Fatigue, bradycardia, insomnia |
| Kerlone | Betaxolol | Selective β1 blocker | Bradycardia, tiredness, visual disturbances |
Non-Selective Beta-Blockers (β1 + β2 Blockers) |
|||
| Inderal | Propranolol | Non-selective β1 & β2 blocker → ↓ HR, contractility; bronchoconstriction (also used for migraines, anxiety) | Bronchospasm, fatigue, depression, cold extremities |
| Corgard | Nadolol | Non-selective β-blocker (long-acting) | Dizziness, fatigue, bradycardia |
| Blocadren | Timolol | Non-selective β-blocker | Fatigue, dizziness, bronchospasm |
| InnoPran XL | Propranolol (ER) | Non-selective β-blocker → long-acting formulation | Hypotension, vivid dreams, cold hands/feet |
Mixed Alpha/Beta Blockers |
|||
| Coreg | Carvedilol | Blocks β1, β2, and α1 → ↓ HR and vasodilation (also blocks α₁ receptors (vasodilation) | Orthostatic hypotension, dizziness, weight gain |
| Trandate, Normodyne | Labetalol | Blocks β1, β2, and α1 → used in hypertensive emergencies and pregnancy | Dizziness, fatigue, scalp tingling |
Combination Beta-Blocker |
|||
| Ziac | Bisoprolol + Hydrochlorothiazide | β1-blocker + Thiazide diuretic | Dizziness, electrolyte imbalance, fatigue |
| Corzide | Nadolol + Bendroflumethiazide | Non-selective β-blocker + Thiazide diuretic | Hypokalemia, bradycardia, hypotension |
| Lopressor HCT | Metoprolol tartrate + Hydrochlorothiazide | β1-blocker + Thiazide diuretic | Dizziness, dehydration, bradycardia |
| Tenoretic | Atenolol + Chlorthalidone | β1-blocker + Thiazide-like diuretic | Fatigue, low potassium, cold extremities |
How Beta Blockers Work
Simple mechanism of Action: Target Receptors:- Beta-blockers primarily block β1 receptors in the heart.
- Some also block β2 receptors in the lungs and blood vessels.
- 🧡 Slower heart rate → less work for the heart
- 💪 Reduced force of contraction
- 🩸 Lower blood pressure
- 🧪 Decreased renin release from kidneys → helps control blood volume and pressure
- Less strain on the heart
- Improved oxygen balance
- Lower blood pressure
- Control of abnormal heart rhythms
Types of Beta Receptors:
| Receptor | Location | Action When Stimulated | What Beta-Blockers Do |
| β1 | Heart, kidneys | ↑ Heart rate, ↑ Renin secretion | ↓ Heart rate, ↓ BP |
| β2 | Lungs, blood vessels | Bronchodilation, vasodilation | (If blocked) Bronchoconstriction |
| α1 (some BBs) | Blood vessels | Vasoconstriction | Vasodilation (when blocked) |
Clinical Effects of Beta-Blockers
| Effect | Clinical Use |
| ↓ Heart rate |
Tachycardia, Atrial fibrillation
|
| ↓ Blood pressure | Hypertension |
| ↓ Myocardial oxygen demand | Angina, Post-MI |
| ↓ Arrhythmias |
Ventricular and supraventricular arrhythmias
|
| ↓ Cardiac remodeling |
Heart failure (e.g., metoprolol, carvedilol)
|
| ↓ Tremors, anxiety |
Essential tremor, performance anxiety
|
| ↓ Intraocular pressure (some) |
Glaucoma (e.g., timolol eye drops)
|
- Less effective than ACEIs/ARBs/CCBs in reducing stroke risk.
- Metabolic effects (may worsen insulin resistance, lipids).
- Side effects (fatigue, erectile dysfunction, cold extremities).
- Exceptions (Preferred Beta-Blockers for HTN) Nebivolol (better vasodilation, fewer metabolic effects).
- Carvedilol (α-blockade helps peripheral perfusion).
Centrally Acting Antihypertensive Agents
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
| Catapres | Clonidine | Stimulates central α2-adrenergic receptors – ↓ sympathetic outflow -↓ BP | Drowsiness, dry mouth, rebound hypertension, constipation |
| Catapres-TTS | Clonidine (transdermal patch) | Same as oral clonidine | Skin irritation, sedation, dry mouth |
| Aldomet | Methyldopa | Converted to α-methylnorepinephrine → stimulates central α2-receptors | Sedation, depression, hemolytic anemia, liver toxicity |
| Tenex | Guanfacine | Central α2-agonist (longer half-life than clonidine) | Drowsiness, dry mouth, fatigue |
| Kapvay | Clonidine (ER) |
Stimulates central α2-adrenergic receptors –
↓ sympathetic outflow – ↓ BP
(used in ADHD but also affects BP) |
Drowsiness, dry mouth, rebound hypertension, constipation |
| Intuniv | Guanfacine ER | Drowsiness, dry mouth, fatigue | |
Combination Products Containing Centrally Acting Agents |
|||
| Clorpres | Clonidine + Chlorthalidone | Clonidine: central α2-agonist + Chlorthalidone: thiazide diuretic | Dry mouth, drowsiness, electrolyte imbalance, dizziness |
| Methyldopa HCT | Methyldopa + HCTZ | Methyldopa: central α2-agonist + HCTZ: thiazide diuretic | Sedation, hypokalemia, hypotension |
- Rebound Hypertension: Can occur if clonidine is stopped suddenly.
- Methyldopa is safe in pregnancy (commonly used for gestational hypertension).
- These drugs are not first-line agents but may be used in resistant hypertension or special populations.
How Centrally Acting Hypertensives Work
- Target Site: These drugs act on the brainstem, specifically areas that control blood pressure.
- Receptor Activation: They stimulate α2-adrenergic receptors in the central nervous system.
- Reduced Sympathetic Outflow:
- This decreases nerve signals that normally cause the heart and blood vessels to work harder.
- Result: Heart rate and blood vessel resistance decrease.
- Outcome:
- Blood vessels relax (vasodilation)
- Heart rate slows down
- Blood pressure drops
- Clonidine binds to α2 receptors in the brain.
- This reduces the release of norepinephrine (a stress hormone that increases BP).
- Less norepinephrine = less stimulation of the heart and arteries = lower blood pressure.
Affects of Centrally acting Hypertensive on Body:
- ↓ Sympathetic nerve signals leads to ↓ Blood pressure
- ↓ Heart rate leads to ↓ Cardiac output
- ↓ Peripheral vascular resistance leads to ↓ Afterload on the heart
- Rebound hypertension (Avoid sudden withdrawal, must taper clonidine).
- CNS depression (drowsiness, impaired concentration).
- Methyldopa: False + Coombs test, rare hepatotoxicity. Monitor LFTs, CBC
Vasodilators
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
| Apresoline | Hydralazine | Directly relaxes arteriolar smooth muscle → ↓ peripheral resistance | Reflex tachycardia, headache, flushing, fluid retention, lupus-like syndrome |
| Loniten | Minoxidil | Opens K⁺ channels in arteriolar smooth muscle → hyperpolarization & vasodilation | Hypertrichosis, edema, tachycardia, pericardial effusion |
| BiDil | Hydralazine + Isosorbide dinitrate | Hydralazine: arteriolar vasodilation; Isosorbide: venous vasodilation | Headache, dizziness, hypotension, drug-induced lupus (hydralazine) |
| Nitropress | Sodium nitroprusside (IV) | Releases nitric oxide → increases cGMP → vasodilation of arteries and veins | Hypotension, cyanide toxicity (with prolonged use), reflex tachycardia |
| Nitroglycerin (IV) | Nitroglycerin | Venous > arterial dilation via NO → ↓ preload and myocardial oxygen demand | Headache, hypotension, flushing, tolerance with continuous use |
| Trandate | Labetalol (has vasodilatory effects) | Mixed α1 and β-blocker → decreases BP via vasodilation and reduced HR | Dizziness, fatigue, orthostatic hypotension, bronchospasm |
| Coreg | Carvedilol (has vasodilatory effects) | Non-selective β-blocker + α1-blocker – ↓ HR and vasodilation | Bradycardia, dizziness, orthostatic hypotension, weight gain |
Notes:
- Hydralazine and minoxidil are often used with diuretics and beta-blockers to counter fluid retention and reflex tachycardia.
- BiDil is specifically approved for heart failure in African American patients.
- Vasodilators are not first-line for essential hypertension but are valuable in resistant hypertension or hypertensive emergencies (IV forms).
Types of Vasodilators
A. Direct Vasodilators
- Arterial Dilators (↓ afterload):
- Hydralazine
- Minoxidil (also causes hair growth)
- Venous Dilators (↓ preload):
- Nitroglycerin (used in angina)
- Isosorbide dinitrate/mononitrate
- Mixed (Arterial + Venous):
- Sodium Nitroprusside (IV for emergencies)
B. Indirect Vasodilators (Other drug classes with vasodilatory effects)
- Calcium Channel Blockers (e.g., Amlodipine)
- ACE Inhibitors/ARBs (reduce angiotensin II effects)
- Alpha-Blockers (e.g., Doxazosin)
Vasodilators Mechanism of Action (Basics)
Vasodilators are medications that help dilate (widen) blood vessels, leading to a decrease in blood pressure. This happens because they relax the smooth muscle in the blood vessel walls, allowing the blood to flow more freely. Let’s break down the process:
Direct Smooth Muscle Relaxation
- Vasodilators act directly on the smooth muscle cells that line blood vessels.
- By relaxing these muscles, the blood vessels widen, reducing the resistance that the heart has to pump against (known as afterload).
- This process decreases blood pressure and improves blood flow to organs and tissues.
2. Nitric Oxide (NO) Pathway
- Some vasodilators (e.g., nitroglycerin, sodium nitroprusside) work by increasing the production of nitric oxide (NO) in the endothelial cells (cells lining the blood vessels).
- Nitric Oxide activates an enzyme called guanylate cyclase, which increases levels of cyclic GMP (cGMP) inside smooth muscle cells.
- This process leads to smooth muscle relaxation and subsequent dilation of blood vessels.
3. K⁺ Channel Opening (Hyperpolarization)
- Minoxidil and hydralazine work by opening potassium channels in the vascular smooth muscle cells.
- The opening of K⁺ channels leads to hyperpolarization (making the inside of the cell more negative), which reduces the ability of the muscle to contract, causing relaxation and dilation of the blood vessels.
4. Sympathetic Nervous System Influence
- Some vasodilators (like labetalol and carvedilol) also have a dual effect, acting as both alpha-blockers and beta-blockers.
- They block alpha-1 adrenergic receptors (which are responsible for vasoconstriction) and beta receptors (which control heart rate and contractility). This reduces the overall sympathetic nervous system activity, leading to decreased vascular resistance and lower heart rate.
Types of Vasodilators and Their Specific Mechanisms:
- Hydralazine: Direct arteriolar vasodilator; increases cGMP levels, leading to smooth muscle relaxation.
- Minoxidil: Opens K⁺ channels in smooth muscle, causing hyperpolarization and vasodilation.
- Sodium Nitroprusside: Releases nitric oxide (NO), leading to both arterial and venous dilation.
- Nitroglycerin: Primarily venodilator; releases NO to relax vascular smooth muscle.
- Labetalol and Carvedilol: Mixed alpha and beta blockers, which lead to both vasodilation and reduced heart rate.
Diuretics
| Brand Name | Generic Name | Mechanism of Action | Side Effects |
Thiazide Diuretics |
|||
| Microzide | Hydrochlorothiazide |
Inhibits Na⁺/Cl⁻ reabsorption in distal convoluted tubule |
Hypokalemia, hyponatremia, hyperuricemia |
| Hygroton | Chlorthalidone | ||
| Lozol | Indapamide | Thiazide-like, inhibits Na⁺ reabsorption | |
| Zaroxolyn | Metolazone | Thiazide-like, potent when combined with loop diuretics | Electrolyte disturbances, dehydration |
Loop Diuretics |
|||
| Lasix | Furosemide |
Inhibits Na⁺/K⁺/2Cl⁻ symporter in thick ascending limb of loop |
Hypokalemia, ototoxicity, dehydration |
| Bumex | Bumetanide | ||
| Demadex | Torsemide | ||
| Edecrin | Ethacrynic acid | Loop diuretic without sulfa group | Ototoxicity, GI effects |
Potassium-Sparing Diuretics |
|||
| Midamor | Amiloride |
Blocks epithelial Na⁺ channels in distal tubule |
Hyperkalemia |
| Dyrenium | Triamterene | Hyperkalemia, nephrolithiasis | |
Potassium-Sparing Diuretics – Aldosterone Antagonists |
|||
| Aldactone | Spironolactone | Blocks aldosterone receptors in distal nephron | Gynecomastia, hyperkalemia, menstrual changes |
| Inspra | Eplerenone | Selective aldosterone blocker | Hyperkalemia, less endocrine side effects |
Combination Diuretic Drugs |
|||
| Dyazide, Maxzide | Triamterene + Hydrochlorothiazide |
Na⁺ channel blocker + thiazide |
Hyperkalemia, hypokalemia, dizziness |
| Moduretic | Amiloride + Hydrochlorothiazide | Hyperkalemia, nausea | |
| Aldactazide | Spironolactone + Hydrochlorothiazide | Aldosterone antagonist + thiazide | Electrolyte imbalance |
| Lasilactone (EU/India) | Spironolactone + Furosemide | Aldosterone antagonist + loop | K⁺ balancing, risk of dehydration |
Diuretics Comparison Table
| Diuretic Type | Site of Action | Main Transporter/Target | K⁺ Sparing? |
| Thiazides | Distal Convoluted Tubule | Na⁺/Cl⁻ symporter | ❌ |
| Loop | Loop of Henle | Na⁺/K⁺/2Cl⁻ symporter | ❌ |
| Potassium-Sparing | Collecting Duct | ENaC (epithelial Na⁺ channel) | ✅ |
| Aldosterone Antag. | Collecting Duct | Aldosterone receptors | ✅ |
How do Diuretics Work
Thiazide and Thiazide-like Diuretics
- Examples: Hydrochlorothiazide (Microzide), Chlorthalidone, Indapamide
- Site of Action: Distal convoluted tubule
- Mechanism:
- Inhibit Na⁺/Cl⁻ symporter, reducing sodium and water reabsorption
- Leads to increased urine output and lower blood pressure
Loop Diuretics
- Examples: Furosemide (Lasix), Bumetanide, Torsemide
- Site of Action: Thick ascending limb of the loop of Henle
- Mechanism:
- Inhibit Na⁺/K⁺/2Cl⁻ symporter
- Causes massive sodium, chloride, and water loss
Potassium-Sparing Diuretics
- Examples: Amiloride, Triamterene
- Site of Action: Collecting ducts
- Mechanism:
- Block epithelial sodium channels (ENaC), reducing sodium reabsorption
- Prevent potassium excretion
Aldosterone Antagonists (also potassium-sparing)
- Examples: Spironolactone (Aldactone), Eplerenone
- Site of Action: Collecting ducts
- Mechanism:
- Block aldosterone receptors
- Reduce sodium reabsorption and potassium excretion
Source
Diuretics Side Effects & Managing or Resolving Those Issues
| Side Effect | Drug Examples | Why It Happens | Solution / Management |
Thiazide Diuretics |
|||
| Hypokalemia (low K⁺), Muscle spasms |
Hydrochlorothiazide,
Chlorthalidone |
↑ K⁺ loss in urine | Add potassium-rich foods or potassium supplements; combine with K⁺-sparing diuretic |
| Hyponatremia (low Na⁺) | Excess sodium loss | Monitor Na⁺, adjust dose, ensure adequate sodium intake | |
| Hyperuricemia / Gout | ↓ uric acid excretion | Use with caution in gout patients; consider alternative | |
| Hyperglycemia | Thiazides reduce insulin sensitivity | Monitor blood sugar in diabetic/pre-diabetic patients | |
| Hypercalcemia | ↓ calcium excretion | Monitor calcium levels, especially in hyperparathyroidism | |
| Erectile dysfunction | Unknown mechanism | Discuss alternatives if needed | |
Loop Diuretics |
|||
| Severe hypokalemia |
Furosemide,
Torsemide |
High K⁺ excretion | Add potassium supplements or combine with K⁺-sparing agent |
| Dehydration | Excess fluid loss | Monitor fluid status, adjust dose, encourage hydration | |
| Ototoxicity | High doses / fast IV push | Avoid rapid IV push; use lowest effective dose | |
| Hypocalcemia, Hypomagnesemia | Increased Ca²⁺ and Mg²⁺ loss | Supplement as needed; monitor labs | |
| Orthostatic hypotension | ↓ blood volume | Rise slowly from sitting/lying; adjust dose | |
Potassium-Sparing Diuretics |
|||
| Hyperkalemia |
Amiloride,
Triamterene |
Blocks K⁺ excretion | Monitor K⁺, avoid in renal failure or with ACE inhibitors/ARBs |
| Nausea, dizziness | General drug effects | Take with food, monitor for symptoms | |
Potassium Sparing Diuretic – Aldosterone Antagonists |
|||
| Hyperkalemia |
Spironolactone,
Eplerenone |
↓ aldosterone = ↓ K⁺ excretion | Monitor K⁺ and renal function |
| Gynecomastia (Spironolactone) | Hormonal effects | Switch to Eplerenone (less hormonal effects) | |
| Menstrual irregularities | Hormonal disruption | Monitor and assess patient concern | |